



Abortion and Women's Healthcare
Pregnancy is becoming a more risky experience
Mea culpa … the article below was accidentally posted prematurely before I had the author’s permission. She has now generously granted permission to share it. JW
Author warning: Without the protections of Roe vs Wade, we are becoming essentially two nations: a first-world nation where it’s relatively safe to become pregnant, and a third-world nation where it’s very dangerous to become pregnant (unless there’s a nationwide ban, in which case pregnant women will all move into a higher-risk stratum). — Elaine Pearce, MD, MHP

(Copyrighted images throughout; for personal, fair use only.)

At its baseline (even before Roe v. Wade overturned), the US was a relatively dangerous place to be pregnant, with maternal mortality rates far higher than other advanced, developed nations. The answer to why is easy: access to care.

Maternity care deserts are places where pregnant women have to drive for long distances to obtain basic prenatal care, treatment for obstetric emergencies and to find places to deliver their babies. As you might expect, outcomes are worse in these regions. Maternity Care Deserts, 2023 (Source: March of Dimes, 2022-3) Dimes)
There are two places where these mainly exist: rural areas (lower population density, fewer resources) and poorer parts of the country, such as the Deep South and Appalachia.
Given that we know we have poor outcomes and that services are unevenly distributed, what are we doing about this?

Answer: nothing. It’s getting worse at a rapid clip. The reason for this is that, unlike all other advanced societies, we don’t view healthcare as a basic human right, we view it as a business. Maternity care centers (aka Labor and Delivery centers, or L and Ds) are money losers – they need to be staffed 24/7 even when there are no patients, and delivering moms are often poor or uninsured. Since an increasing number of American hospitals are run by for-profit corporations, when the question is asked, “Which departments are under-performing?” the answer is obvious and L&Ds get axed.
Roe v. Wade, the landmark Supreme Court case 1973 – June, 2022
For almost 50 years, this case protected a woman’s Constitutional right to an abortion. Note: Roe v. Wade was not a carte-blanche approval. For each trimester, the criteria got stricter, with third-trimester abortions limited to being essential to protect the life or health of the mother.
Dobbs vs. Jackson Women’s Health Organization. Within 6 months, 15 states had banned abortion, with more states banning or restricting it since. The deciding votes were cast by the three Supreme Court justices that Donald Trump appointed. Multiple states rushed to ban or severely restrict the procedure.
Current Abortion Bans and Restrictions

Over one third of American females lives in states with bans or restrictions. Very few women know that they are pregnant at 6 weeks, so in effect 6-week bans are full bans.
Note that there has been an attempt to confuse the public by switching between terms such as “bans,” “restrictions,” and “limitations.” In each case, the definiCon of the term in that context needs to be understood (and is often not explained). “Donald Trump will oppose a national abortion ban,” (per JD Vance) does not exclude the possibility of a national abortion “restriction” at 6 weeks, which, as explained, will turn out to be a total ban for the vast majority of women.
If you want continuously updated info on what individual states are up to on this issue, go to After Roe Fell: Abortion Laws by State.

A critical thing to understand is that if a woman seeks to terminate her pregnancy, the procedure is called an “abortion”. If she is having a miscarriage, the procedure is called a “D and C” (dilation and curettage). They are the exact same procedure (except for late miscarriages, when a dilation and evacuation procedure may be used instead). A doctor in an abortion-ban state, therefore, has the potential of facing 12 jurors, none of whom likely have medical training (and with the possibility that some of them are anti-abortion activists looking to make a statement), and trying to convince them that s/he was doing a D&C for a woman having an inevitable miscarriage vs. an illegal abortion for a woman who was just having some temporary bleeding during an otherwise uneventful pregnancy. An unlucky throw of the dice means, not just the end of a career, but a prison term.
Consider a hypothetical patient, Sue, who lives in an abortion ban state. She is 12 weeks pregnant and is having heavy bleeding with some cramping. She sees her PCP, Dr. Smith, who does a cursory exam and tells her she’s probably just “spotting” and it may well settle down. A few days later, she develops increasing abdominal pain and thinks she saw some tissue with the blood in the toilet bowl. She goes to the ER. The doctor there finds normal vital signs and blood work and a detectable fetal heartbeat by ultrasound. They tell her that it’s too early to do anything, so she’ll have to wait and see. “Make an appt. to see your PCP.” A few days after that, she’s having excruciating pain, fever and shaking chills. She goes to the ER again; this Time she’s orthostatic (her standing blood pressure is low), she has an elevated white blood cell count (showing systemic infection) and there is no longer a fetal heartbeat.
At this point, Sue has satisfactorily demonstrated that she is having an inevitable miscarriage and her doctors are no longer worried about going to prison. Best case scenario is that a simple, outpatient procedure has been converted into an expensive hospital stay, possibly requiring invasive care that will reduce her future fertility. Worst case scenario is that they waited too long and she dies. We are already reading reports of this kind of medical brinksmanship in abortion ban states.
That was a hypothetical. Here are some real-world examples:
Bleeding and in pain, she couldn't get 2 Louisiana ERs to answer: Is it a miscarriage?
Idaho's biggest hospital says emergency flights for pregnant patients up sharply

The maternal mortality consequences of losing abortion access
The University of Colorado study that projected a 24% mortality increase* during pregnancy looked at mortality results under a national abortion ban if all other conditions remained the same. In actuality, multiple other conditions would change under such a ban, for example, increased illegal abortions, increased maternity care deserts, increased poverty and malnutrition leading to poor outcomes (due to the expense of childrearing and employment loss due to unplanned pregnancies), etc. These additional factors would further raise maternal mortality. (*estimated numbers of deaths/yr are 861 to 1071 nationally … a 24% increase).
Here’s another study – this one compared maternal mortality in highly restrictive states with less restrictive states. Even after correcting for identifiable confounding variables, the highly restrictive states had higher maternal mortality. (No specific variable for living in a maternity care desert was available, but living in an urban area was controlled for.)

Ectopic (tubal) pregnancies develop in the Fallopian tube – these never result in a live birth, and when the tube inevitably ruptures, internal bleeding can kill the woman within a couple of hours. The formerly high mortality of this condition has been brought down remarkably by recognizing it as the medical emergency it is and developing protocols for rapid diagnosis and treatment.
Two women (who don’t know each other) are suing the state of Texas because they sought emergency care repeatedly and were not only not told of the diagnosis, but sent home without treatment. They both had to leave the state to get care for their conditions, creating considerable delay. Due to being treated after tubal rupture, they both had to have salpingectomies (tube removal) which reduces their future fertility.
This happened even though Texas law (in the small print) says that treatment for ectopic pregnancies is legal. Their doctors/hospital administrators were so freaked out and so ignorant of the new laws that they committed gross malpractice (unsurprising when physicians face a potential penalty of life in prison).
There are an estimated 50,000 emergency room visits for ectopic pregnancies per year in the US – this is not a rare problem. To see the murkiness and variability of “exception” clauses in State bans, read this.
Politifact tries to clear up rampant confusion about ectopic pregnancies:
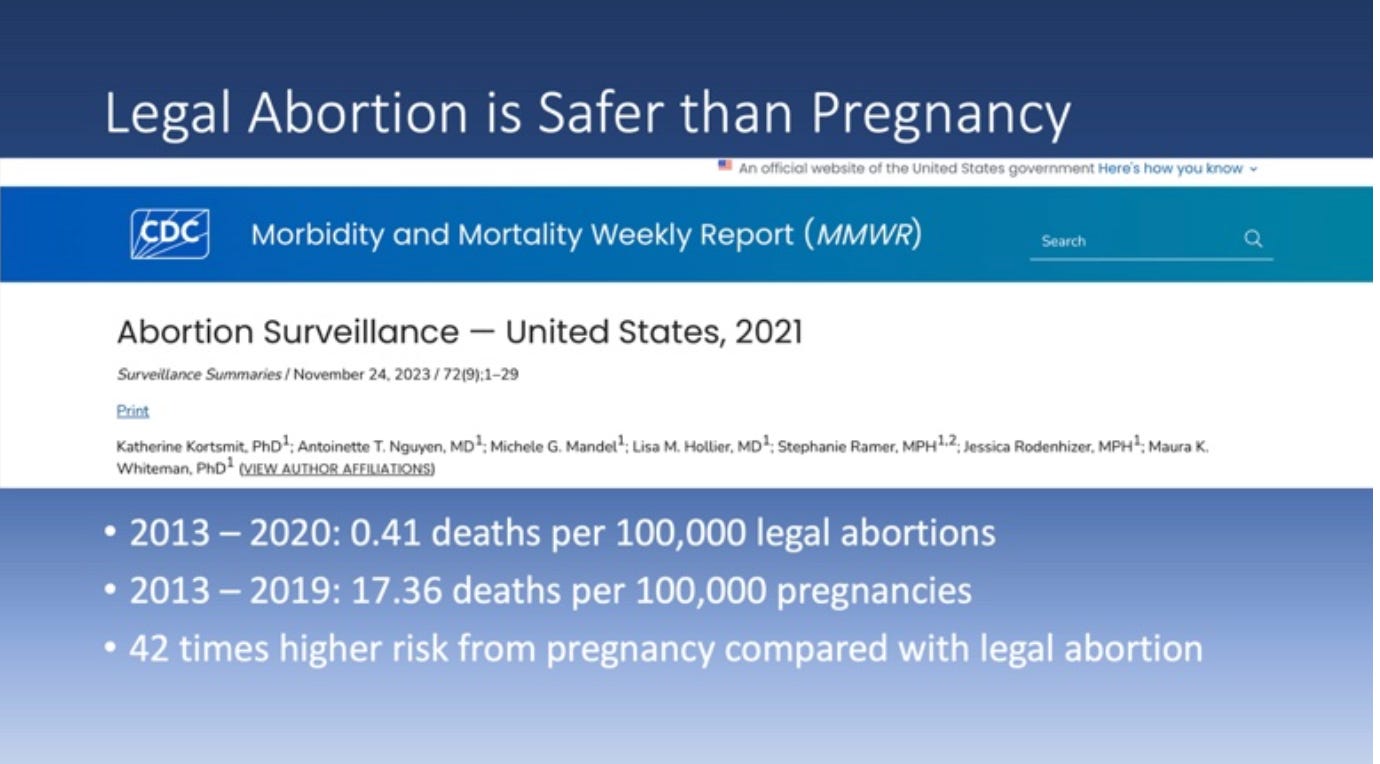
Some people opposed to abortion claim that their main concern is to save the lives of women who will be physically harmed by the procedure. As you can see from the CDC data above, a woman is much more likely to die if she carries a pregnancy to term than if she gets a legal abortion, so this argument is invalid. Note that abortion deaths are so low that the number is presented in a multiple year range, not by individual year. For pregnancy deaths, I chose to leave out 2020 because pregnant women had a higher COVID death rate than nonpregnant women that year, making the ratio look even worse.

Note the marked geographical disparity in maternal death rates – the map on the right is from before the Dobbs decision. When we see the similar distribution of the abortion ban states, it tells us that there will be cumulative, additive effects on maternal mortality. We will essentially become two nations: a first-world nation where it’s relatively safe to become pregnant, and a third-world nation where it’s very dangerous to become pregnant (unless there’s a nationwide ban, in which case we’ll all move to a higher-risk stratum).
Now, we’ll look at two types of high-risk conditions for pregnancy: age and race.

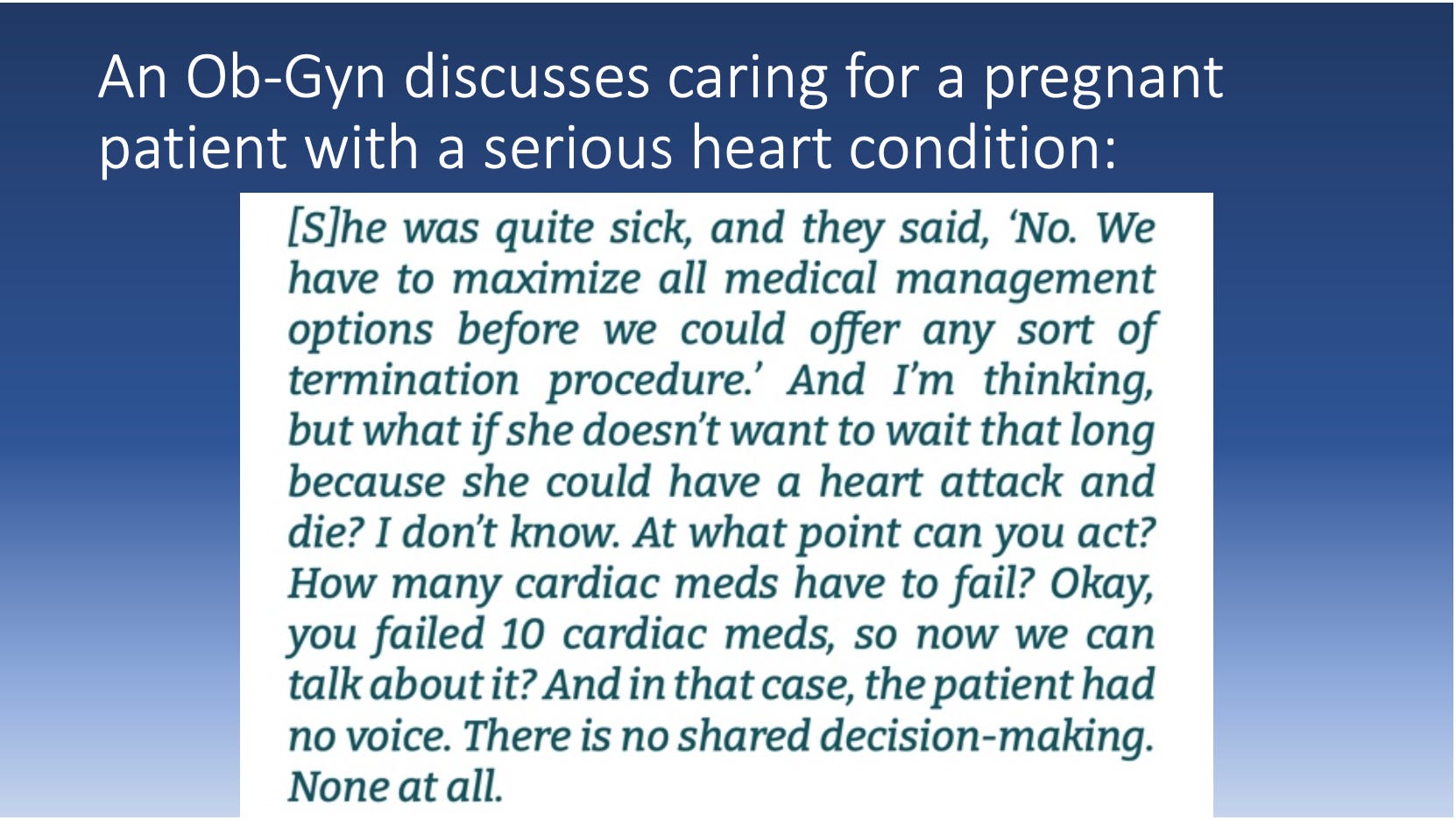
Over the age of 40, maternal mortality is, on average, 7 times the mortality of pregnant women under 25. How many older women, especially those with chronic illness and therefore at even higher risk of a poor outcome than their same-age cohorts, will be surprised by a contraceptive failure or the fact that their menopausal symptoms did not mean they were incapable of becoming pregnant? Quantifying the mother’s risk will always be somewhat a matter of conjecture and therefore, legally unspecified. Doctors will have to weigh the risks they’re willing to take with their personal freedom vs. providing the best care for the mother. An example of this kind of case follows, excerpted from the document shown below.


As we’ve seen, Black women are more likely to live in maternity care deserts, and be impacted by poverty, which means they often don’t get the preventive prenatal care that would lower maternal morbidity/mortality. The University of Colorado study cited earlier predicts, in the case of a national abortion ban, a 39% increase in Black maternal mortality would occur (293 to 406 deaths/yr). This increase is on top of the nation’s already severe racial disparities.
Many low-income Black women already live in what is essentially a national abortion ban.

Fetal abnormalities such as these often cause miscarriages, but in the case that the infant is born alive, he/she dies within days, if not hours, of birth. Should a woman have to know for months that the fetus growing within her is destined to die immediately after birth? Abortion ban proponents say, “YES.” Studies of the psychological impact of bearing these pregnancies show that it is as bad as you would think it is.
Physicians are discussing amongst themselves the moral distress they’re facing. As one put it, “We can tell a patient that their pregnancy is impacted by a fetus that has no brain or skull, but we can’t offer them termination of that pregnancy in Tennessee.” Abortion Bans Are Creating OB-GYN Residency Deserts Across the Country
More mutual hand-wringing amongst physicians. “No one wants to be that test case” (of a doc going to prison, that is). What doctors should know about emergency abortions in states with bans

A few of the hundreds of changes it recommends to overhaul the Federal government are listed here. After this document’s proposals made it politically radioactive, Trump claimed not to know it existed. So do we still need to pay attention to it? YES. (BTW, Kevin Roberts is the head of the Heritage Foundation.)
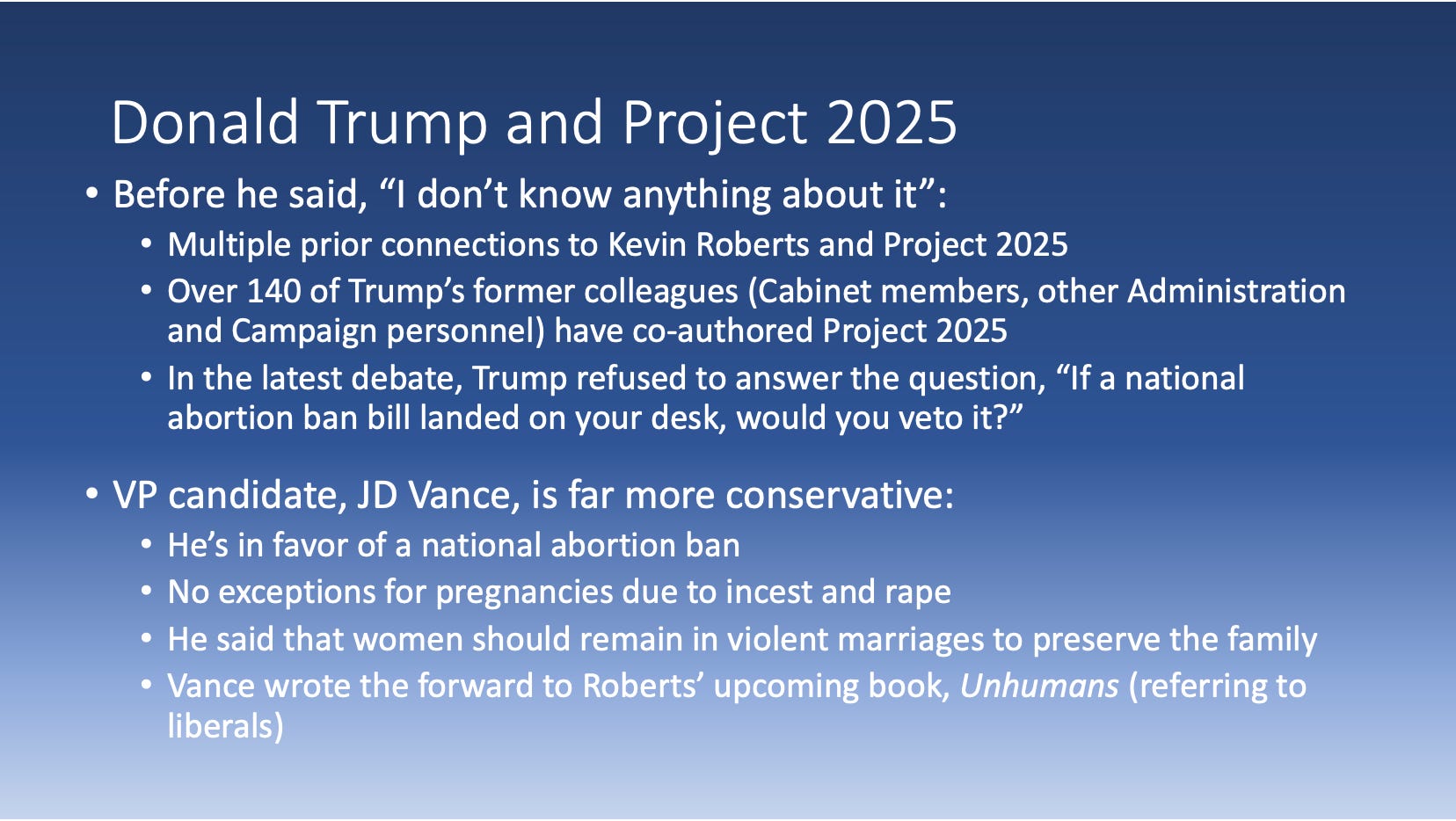
These two men could wind up in charge of the healthcare decisions made for over 150 million women and girls for years to come. JD Vance’s views are important because, given Trump’s age, Vance could easily wind up president, either during the next 4 years or in 2029.

Fortunately, you don’t have to slog through its 900+ pages. The wonderful website www.25and.me allows you to look up your topic of interest and it will point you to every place where the topic is mentioned. It gives you a summary and if you click on the page number, you can read the full passage. This is just a portion of the instances that reproductive health care is discussed. There are a lot of head-exploding proposals in here; I will highlight two of them.
Top arrow: hospitals can refuse to provide emergency abortion care. “Emergency” means “to save the life of the mother.” This violates the Hippocratic Oath, EMTALA Federal law (that mandates that all patients receive stabilizing care in ERs), and basic human decency. Project 2025 seeks to reinterpret EMTALA so that stabilizing care refers primarily to the fetus, not the mother – in the hierarchy of care, the mother is at the bottom.
Bottom arrow: A mandatory national database will be created containing the outcomes of all pregnancies. This will create a surveillance state enabling law enforcement to hunt for women and providers to prosecute. This data can be shared with abortion ban states, enabling women who had abortions to be prosecuted even if they had the procedures done in states where it was legal.
Much has been made of the fact that nowhere in Project 2025 is the term “national abortion ban” mentioned. But by repurposing the Comstock Act to ban the transport of abortion medications and surgical implements across state lines, Project 2025 will create a functional national abortion ban.

“Abortion is not health care” is the mantra of Project 2025, in an adempt to convince the public that abortions are always done on a whim or for convenience.
The case that changed Ireland, a Catholic, anti-abortion country
They might not want to say that to the family of the late Irish dentist, Savita Halappanavar. She presented to an Irish hospital with serious complications of her 17-week pregnancy. When she asked if termination could be considered, she was told “No, because we are a Catholic country.” She proceeded to get sicker in the hospital, developed septic shock and died at the age of 31. Widespread outcry and protest marches after her death led Ireland to change its Constitution and make abortion legal. This most anti-abortion of countries has adopted common sense and moved forward. We are moving backward.
What is happening around the world recently? A broad push to liberalize abortion laws in over 60 nations. The US is one of only four countries that have regressed – we are in league with El Salvador, Nicaragua, and Poland. The World’s Abortion Laws
Is abortion health care? Here’s what ACOG, the premier medical authorities in the US have to say about it. (Note: to be a Board-certified OB-GYN, you need to pass ACOG’s exam.):

The Society of Maternal-Fetal Medicine, the American Medical Association, and other professional organizations also support this position.

The Roe vs. Wade case was Democracy in action: it reflected the will of the majority of Americans. When people are asked (even in conservative Kansas) they resoundingly say that a woman’s healthcare decisions should be left to her and her doctor.
Abortion opponents are working hard to silence the people’s voice. That’s why anyone who speaks out will be harassed in an attempt to intimidate, both informally by online trolls, and increasingly by legal authorities. Dr. Bernard was adempting to highlight the cruelty of Ohio law, which prevented a young child from being protected from the consequences of rape. The legal actions subsequently taken against Dr. Bernard were not just to silence her; they were a warning intended to silence anyone else who might want to speak out about the conditions that they are witnessing.

Not surprisingly, OB-GYNS, Family Practitioners, and Pediatricians are running for the exits of abortion ban states. OB-GYN training programs in these states are having trouble filling positions, and those who do train in these states will not learn essential skills that could help them save a woman’s life in an emergency. Traditionally, fifty percent of doctors who train in a state, stay to practice in that state. All of these factors will greatly worsen maternity care deserts and drive up maternal mortality.
In fact, New Mexico is cheekily trying to poach medical providers from Texas by putting these billboards all over the Lone Star state:


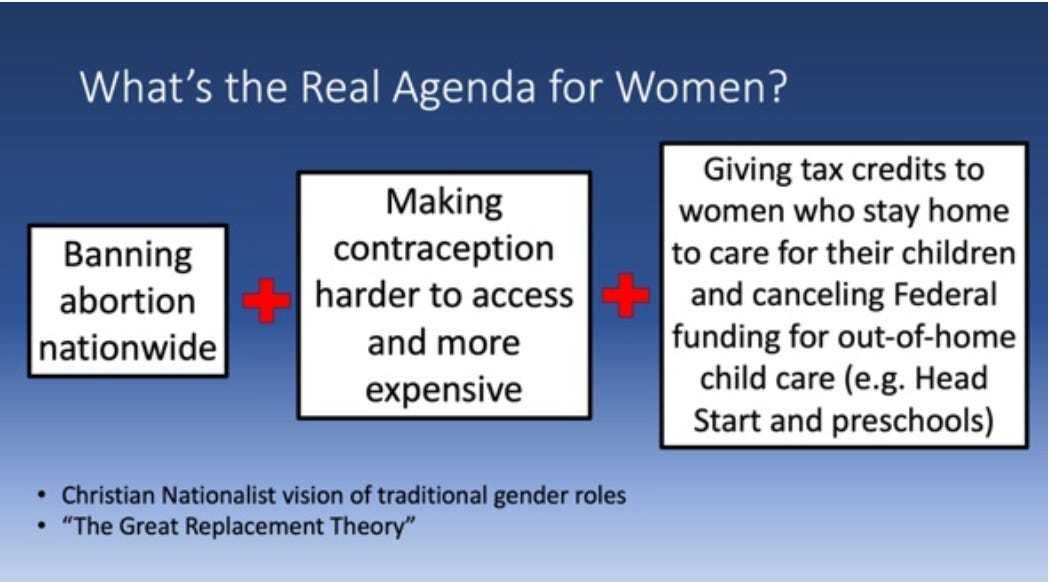
Decades of studies around the world prove this: if you make contraceptives easily and cheaply available, you drive down the demand for abortion. Given Project 2025’s aim of eliminating abortions, this should be a no-brainer. However, the document recommends multiple ways to make contraception harder for women to obtain (and not just for the methods that they claim are abortifacients, like IUDs and morning-after pills).
One wonders why they would promote policies that so undermine a stated goal. The answer can be found in a wider reading of Project 2025. This document is permeated with Christian language and values (particularly Evangelical and conservative Catholic variants where women are viewed principally as homemakers who should have lots of children).
However, in contrast to this nostalgic fantasy, the reality is that American women are a backbone of the workforce outside the home (besides doing a vast majority of the work inside it). So, we might ask the following questions: What happens when women are thoroughly blocked from planning their family’s size and the interval between their children? What happens to the stability and predictability of the workforce? What happens to the American economy?
For the sheer magnitude of the level of responsibility that American women shoulder, compared to the situation in other advanced nations, read this: America’s Social Safety Net: Women

We could argue about whether programs like this one are enough, but does anyone doubt that some Federal oversight is needed, given our enormous regional/class/racial disparities and our for-profit health care system’s abdication of its responsibility to protect maternal health? At least this administration is doing something.

This talk has focused on population-wide effects, but I invite you to consider the future of the women and girls whom you care about: their health, the families that do or will depend on them, their educational and career opportunities, and their economic prosperity. In November, we will be asked to choose between two very different life possibilities for women and girls, outcomes which will last far, far longer than the next 4 years.
And another thing: Project 2025 would "prohibit abortion travel funding." That is, it would stop supporting the financial needs of women who travel from their home states to procure abortions elsewhere.
I am interested in scientifically analyzed data taken from comparable patient groups which establishes that causing fetal demise prior to delivery results in better outcomes for the mother than simply attempting a delivery, when the need arises to address a medical emergency affecting the mother.
The US has the most high risk maternal population (advanced age, chronic use of pharmaceuticals, plus excessive body mass) of any large developed country, and so it is natural that pregnancy outcomes are not good in comparison to countries with similar economic status.
Obstetrics is an unattractive occupation partly due to the high expense of malpractice insurance, which fits the patient population, the quality of practitioners overall, ACOG approved practices, and the liability of being sued for wrongful life as well as wrongful death.
People must adapt themselves to further decreases in available obstetric care as well as all other forms of healthcare as the systems are being taken apart by numerous external forces.
Weight loss for improving health, and improving future pregnancy outcomes should be done by other (dietary) means than GLP1 RAs since these are fraught with side effects, drug interactions, and the problem of weight gain when discontinued.